
Vasopressors are a mainstay of treatment for patients with shock.1 Historically, prolonged or high-dose vasopressors have been administered through central venous catheters (CVCs), a practice that stems from safety concerns following early reports of severe ischemic tissue injury due to peripheral vasopressor extravasation.2–4 Peripheral intravenous (PIV) access in these reports was often via metal cannulae secured with the venous cutdown technique, for example, in the saphenous vein. Vascular access and infusion technologies have since been significantly modernized, but CVCs remain the standard for patients requiring vasopressor therapy at many institutions due to historical beliefs.1
With growing evidence that earlier vasopressor initiation is associated with improved outcomes in shock, there is renewed interest in PIV-based initiation of vasopressors to avoid delays and complications associated with CVC-based placement. Here, we present a narrative review of evidence comparing the safety profiles of CVCs and PIVs for vasopressor administration. Evidence from systematic reviews and meta-analyses, randomized controlled trials (RCTs) and large prospective cohort studies was prioritized in our literature searches, while smaller observational studies were included when they provided unique data (for example, on midline catheters, vasopressin or pediatric populations). We argue that protocolized peripheral vasopressor administration is a reasonable first-line strategy for appropriately selected patients with adequate monitoring and institutional protocols in place. CVCs are appropriate for high-dose vasopressor therapy, the presence of multiple incompatible infusions or when there are other indications for central venous access.
Baseline risks associated with central and peripheral vascular access strategies
Risks associated with central venous catheters
CVC insertion is common and has been the standard of care for patients with shock for decades.1 Other indications for CVCs include hyperosmolar therapies such as high osmolality total parenteral nutrition (TPN), certain chemotherapies and therapeutic/monitoring technologies, such as pulmonary artery catheterization and transvenous cardiac pacing. Despite their utility and importance, CVC insertion carries immediate procedural risks and introduces later risks of infectious and thrombotic complications.5 Moreover, CVC insertion takes time and may delay the initiation of time-sensitive therapies, including vasopressors.6
In a recent systematic review and meta-analysis of 130 studies published between 2015 and 2023, data from over 214,000 catheters were used to evaluate complication rates for modern vascular access.5 The estimated risk of at least one major complication (arterial cannulation, pneumothorax, infection or deep vein thrombosis [DVT]) for patients with a CVC in place for 3 days was approximately 3%.5 Insertion-related complications, including placement failure and arterial puncture, occurred at a pooled rate of 20.4 per 1,000 catheters and 16.2 per 1,000 catheters, respectively. More severe events, including arterial cannulation (2.8 per 1,000) and pneumothorax (4.4 per 1,000), also occurred frequently, although wide prediction intervals reflected major heterogeneity across studies.5 The use of point-of-care ultrasonography (POCUS) for insertion was associated with a lower risk of arterial puncture and pneumothorax.5 Downstream risks were also evaluated: the pooled incidence of central line-associated bloodstream infection (CLABSI) was 4.8 per 1,000 catheter-days, and DVT occurred at a rate of 2.7 per 1,000 catheter-days.5
Risk associated with peripheral intravenous-based vasopressor delivery
There remains a paucity of randomized evidence evaluating PIV-based vasopressor administration (with rare exceptions), such that the strongest evidence summarizing the rate of complications associated with the use of PIV-delivered vasopressors comes from systematic reviews and meta-analyses (Table 1).7–10 These studies highlight that the incidence risk of complications from PIV-based vasopressor administration is low, occurring at a rate of 1–6%. Importantly, when complications do occur, they are typically localized tissue reactions of low severity, such as extravasation, edema, erythema, phlebitis, discomfort or skin blanching. These minor events can be either monitored with no need for intervention or treated with local application of vasodilators such as subcutaneous phentolamine and topical nitroglycerin paste. Major complications, such as thrombophlebitis, were identified infrequently. Serious complications, such as severe necrosis, tissue injury or compartment syndrome, were rare, with two cases of ischemia and skin necrosis each reported in a pediatric and an adult study.11,12
Table 1: Summary of systematic reviews and meta-analyses for risks associated with peripheral vasopressor delivery7–10
| Author (year) | Population | N, studies | N, population | % NE | Risk of complications (overall) | Rate of complications (major/severe) | Rate of complications (minor) |
| Tran et al. (2020)7 | ICU and ER; mixed shock | 9 | 1,835 adults | 65% | 8.6% (95% CI 3.1–21%) | 0.2% | 6.4% |
| Tian et al. (2020)8 | ICU and HDU; sepsis and shock | 7 | 1,382 adults | 49% | NR | None | 3.4% (95% CI 2.5–4.7%) |
| Owen et al. (2021)9 | ICU, ER and OR; adults and children | 11 (adults) 4 (children) | 16,055 adults 388 children | 97% (adults) NR (children) | 1.8% (95% CI 0.1–4.8%) in adults 3.3% (95% CI 0.0–10.1%) in children | Four events | NR |
| ZhangJian et al. (2026)10 | ICU, HDU, ER, OR and ward | 49 | 33,060 catheters | 70% | NR | 0.0% (95% CI; 0.0–0.0%) | 2.3% (95% CI 1.5–3.7%) |
ER = emergency room; HDU = high dependency unit; ICU = intensive care unit; NE = norepinephrine; NR = not reported; OR = operating room.
Broadly, the available evidence suggests that PIV-based vasopressor administration is largely safe and well tolerated, at least in adults in the acute care setting. Although the overall risk of complications was comparable to the pooled risk of major complications associated with CVCs, major or severe complications were found to be exceedingly rare. Taken together, the available data suggest that PIV-based vasopressor administration is a reasonable alternative to CVC-based infusions in many cases. The low overall risk of complications is likely driven by improved medication administration practices, such as modern PIV catheters, improved placement techniques and improved infusion monitoring and delivery practices.
Several limitations of the evidence supporting the safety of PIV-based vasopressor administration warrant consideration. First, studies evaluating the safety of PIV-based vasopressor administration are predominantly observational. Second, the operational definitions of ‘extravasation’ and of ‘complication’ vary substantially across studies, ranging from any localized erythema or blanching to clinically significant tissue injury. This clinical and methodological heterogeneity complicates the pooling and interpretation of incidence estimates. Third, catheter characteristics (gauge, site and technique of insertion) and monitoring protocols (frequency of nursing assessment, criteria for catheter exchange and availability of antidotes) differ markedly between cohorts and are inconsistently reported, contributing further to the statistical heterogeneity across studies. Fourth, retrospective chart review can be prone to under-ascertainment of minor extravasation events. Finally, most studies enrolled adults receiving relatively short-duration, moderate-dose vasopressor therapy, limiting the inferences that can be drawn for pediatric populations, prolonged infusions, very high doses and patients with multiple concurrent vasoactive agents. Pooled risk estimates from the available meta-analyses should, therefore, be interpreted with appropriate uncertainty, and clinicians should weigh the local applicability of the underlying evidence when designing institutional protocols.
Comparative risk associated with central venous catheter versus peripheral intravenous-based vasopressor delivery
As noted, few studies have directly compared complication rates of vasopressors given by PIV versus those given by CVC. A small multicenter French RCT published in 2013 by Ricard et al. (ClinicalTrials.gov identifier: NCT00122707) randomized 266 adult patients in the ICU to PIV or CVC initial venous access if they required vasopressors, other venotoxic medications (such as vancomycin or amphotericin) and prior difficult PIV access.13 Seventy percent of the patients included in this study met criteria for enrollment based on the need for vasopressor delivery. The incidence rate of major complications was higher in the group randomized to PIV initial access as compared with the CVC group (1.04 versus 0.64 complications per patient, p<0.02). However, this difference was almost entirely driven by difficulties with insertion and maintenance of PIVs and erythema at the site of insertion. There were no differences between groups in major infectious or thrombotic complications, pneumothoraces or arterial punctures, or rates of minor complications. Importantly, 48% (61/128) of patients randomized to the PIV group never received a CVC according to a priori crossover criteria, supporting other estimates of the proportion of patients that might avoid CVC placement by following norepinephrine dose thresholds.14
More recently, a cohort study of patients enrolled in the Crystalloid Liberal or Early Vasopressors in Sepsis (CLOVERS) trial (ClinicalTrials.gov identifier: NCT03434028), conducted in 60 US hospitals from March 2018 to February 2022, assessed complication rates associated with vasopressor delivery via both CVCs and PIVs.15 CLOVERS enrolled 1,563 patients, of which 582 (37.2%) received vasopressors through a known route. Most patients (84.2%) had vasopressors initiated via PIV, with peripheral administration continued beyond 6 h in 333 of 490 patients (68.0%). PIV-associated complications were rare (0.6%, 3/490 participants) and of low severity, while CVC placement-related complications occurred in 12 of 322 patients (3.7%) in the first 72 h. While the risk of complications associated with PIV-based vasopressor administration in this study was low, rates of minor complications may be subject to under-detection due to the use of retrospective chart review.15
Factors that may change baseline risk
Ultrasound guidance
Lower rates of complications have been noted in observational studies that used real-time POCUS guidance during CVC insertion irrespective of site, including pneumothorax, arterial puncture and placement failure.5,16 The greatest benefit of POCUS is likely when it is applied to internal jugular cannulation, for which a substantially lower rate of pneumothorax has been reported (risk ratio, 0.02; 95% credible interval: 0.001, 0.28). POCUS may also be associated with smaller reductions in insertion-related risk of pneumothorax for subclavian cannulation, as well as arterial puncture for both internal jugular and subclavian cannulation.5 These findings support recommendations for the routine use of POCUS, where available, for CVC insertion in clinical practice guidelines from multiple acute care and perioperative societies.17–20
POCUS to facilitate PIV access has also been investigated, primarily for patients with difficult venous access. Meta-analyses of both pediatric and adult studies suggest that POCUS facilitates first-attempt success and may reduce the total number of attempts for PIV cannulation.21–24 Ultrasound-guided PIVs were shown to work best and have the lowest risk of failure over time for shallow vessels (e.g. <0.4 cm depth) and when placed in the antecubital fossa or forearm. However, data on longer term outcomes, such as PIV failure rates over time (i.e. PIV survivability), as well as infiltration or extravasation injury as compared with PIVs placed using standard techniques, are lacking.
Insertion site
The anatomic site used contributes to differences in insertion-related complications and downstream complications of CVCs. In the 3SITES trial (Venous Site for Central Catheterization, ClinicalTrials.gov identifier: NCT01479153), a large multicenter trial of 3,027 patients randomized to receive a CVC in the subclavian, jugular or femoral vein, the primary outcome was a composite of CLABSI and symptomatic DVT.25 Rates of the primary outcome were 1.5, 3.6 and 4.6 events per 1,000 catheter-days in each insertion site arm, respectively. The risk of the primary outcome was significantly higher by pairwise comparison in the femoral group than the subclavian group (hazard ratio [HR], 3.5; 95% CI: 1.5, 7.8; p<0.01) and in the jugular group than the subclavian group (HR, 2.1; 95% CI: 1.0, 4.3; p=0.04).25 Not surprisingly, the risk of major mechanical complications (pneumothorax, arterial injury and hematoma) was lower for the femoral as compared with the subclavian vein (HR, 0.3; 95% CI: 0.1, 0.8; p=0.03) and trended toward lower for the jugular as compared with the subclavian vein (HR, 0.5; 95% CI: 0.3, 1.1; p=0.09). This difference in risk is supported by a meta-analysis showing that subclavian access is associated with a higher rate of pneumothorax compared with internal jugular access (7.8 versus 1.9 events per 1,000 catheters).5
In contrast, few studies have evaluated how complication risk varies by insertion site for PIV-based vasopressor delivery. Conventionally, PIVs placed in the forearm (cephalic, basilic and median cubital veins) are considered safest.26 In two meta-analyses, the site of PIV-based vasopressors administration was not associated with a difference in risk of complications.7,9 Despite a lack of data on complication rates, anatomic factors such as venous diameter, depth of vessel from skin and proximity to joints likely remain important considerations.27 Larger veins, i.e. venous diameter >4 mm, may increase relative dilution of vasopressors and caustic medications and could be less likely to spasm, although data on this are limited.26 Larger veins also tend to be deeper, but deeper vessels may have a higher risk of failure over time when accessed using ultrasound, implying there may be a trade-off between optimizing venous diameter and depth. Intuitively, vasopressors should not be infused through PIVs that cannot be routinely monitored or assessed, or in sites complicated by burns, active infection, edema or abnormal vascular anatomy such as arteriovenous fistulae.
Broadly reflecting these considerations, a survey of hospital vasopressor policies in Michigan found that 53% of the 38 hospitals with a policy governing peripheral administration of vasopressors limited the site for PIV-based delivery, with 100% of these policies prohibiting vasopressor infusion through PIVs in the leg and almost all prohibiting vasopressor infusion through PIV access in the hand or wrist. The forearm was the site prohibited the least often.28 While the antecubital fossa was used in multiple studies showing the broad safety of PIV-based vasopressors, approximately 40% of surveyed Michigan hospitals with peripheral vasopressor policies prohibited vasopressor infusions through the antecubital fossa.28
Peripheral intravenous-specific factors and monitoring
The optimal size of PIV catheters used for vasopressor administration remains unknown. In most studies showing the safety of vasopressors administered via PIV, protocols dictated the use of at least an 18- to 20-gauge catheter, with at least one study allowing 22-gauge catheters.13,29,30 This minimum size requirement seems to be relatively common, with 50% (19/38) of the abovementioned Michigan hospitals surveyed reporting policy limits on peripheral vasopressors on the basis of catheter characteristics and requiring at least an 18- to 20-gauge catheter.28 However, the evidence is mixed. While one meta-analysis reported a significant association between catheter size and the prevalence of complications with a cutoff of 20 gauge, another meta-analysis showed no difference in the incidence of complications between 16- and 20-gauge catheters as opposed to 22–gauge or smaller catheters.7,9 In adults, it seems most prudent to use the largest PIV or at least 20–22-gauge, provided all other PIV-specific factors such as anatomical site are acceptable.
Potentially more important than catheter-specific characteristics are the systems and protocols in place by which they are monitored.31 The prevalence of complications associated with PIV-based vasopressors was lower in studies reporting the use of infusion safety guidelines as compared with those that did not report the use of such guidelines (RR, 0.12; 95% CI: 0.038, 0.30, p=0.02).7 While protocolized monitoring varies between institutions and study protocols, common features dictate requirements for minimum PIV catheter size, ideal and prohibited catheter sites, placement confirmation with ultrasound, quality assessments of catheters by saline flush tests and blood aspiration, limits on duration and dose of infusions and availability of immediate treatment for extravasation (Figure 1).13,29–31
Figure 1: Common criteria for safe peripheral IV vasopressor administration
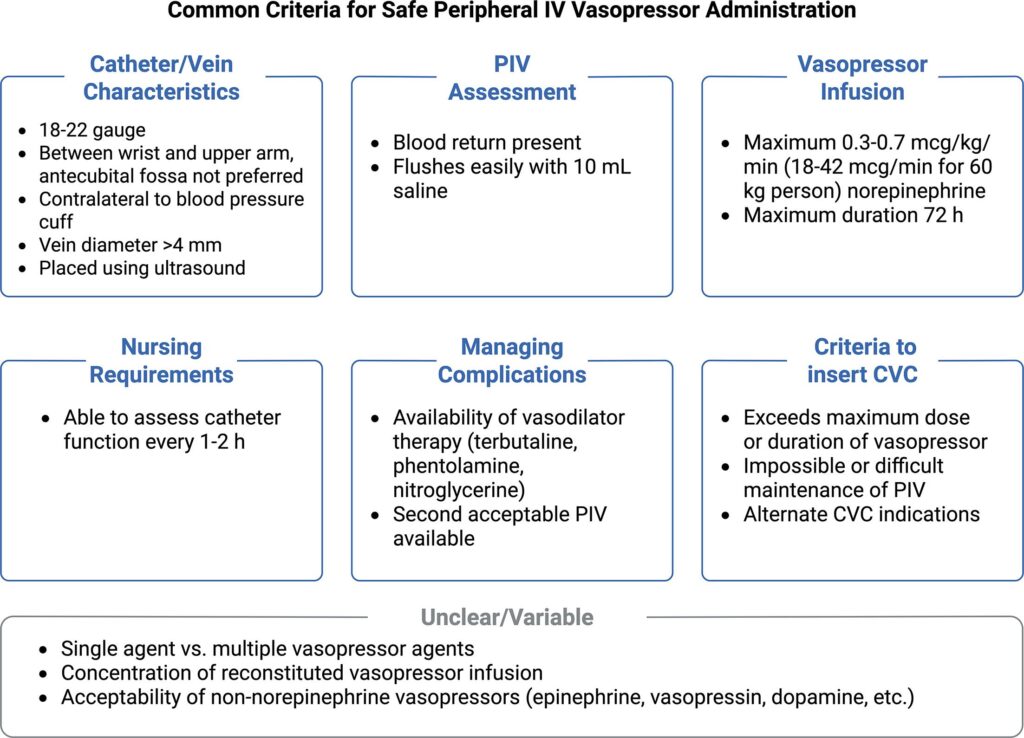
CVC = central venous catheter; IV = intravenous; PIV = peripheral intravenous
Vasopressor exposure and drug
The exposure of local tissue to a drug through a PIV is a function of the required clinical dose (e.g. in µg/kg/min), concentration of the drug infusion (e.g. in µg/mL) and duration of infusion. Although it is generally assumed that high doses or concentrations of vasopressors require a CVC for safe administration, there is a lack of data linking vasopressor doses to PIV-related complications. Peripheral extravasation has been reported across the entire range of reported norepinephrine doses.30,32 Average maximum doses of vasopressors are widely variable when reported in several studies: 0.10–0.70 µg/kg/min (norepinephrine), 1–3.25 µg/kg/min (phenylephrine), 0.06 µg/kg/min (epinephrine) and 0.04–0.06 units/min (vasopressin).8,15,30,33,34 There is a similar lack of data on whether drug concentration contributes to differences in risks associated with PIV-based vasopressors as well. Heterogeneity and nonuniformity of data from observational studies, including lack of reporting and non-weight-based reporting, precluded meta-regression analyses by vasopressor concentrations in four meta-analyses.7–10 The lack of definitive data showing safe dose thresholds is reflected in the relatively low proportion of Michigan hospitals (45%) with policy limits on peripheral vasopressor administration based on dose alone, and concentration limits were not investigated in this study.28
It seems logical that the risk of extravasation would increase with prolonged infusion duration. However, the length of infusion has not been shown to be correlated with higher rates of complications with peripheral vasopressors.8–10 In fact, the majority of extravasation events from PIVs are reported to occur within the first 24 h.29,34 In most observational studies, the average duration of vasopressor infusion via PIV ranges from 1 to 48 h, with 12–24 h being the most common duration reported.8–10 The practice at some of our institutions is not to limit PIV vasopressor delivery based on duration of vasopressor use alone, consistent with a recent implementation study of PIV vasopressor delivery.29
The risk of complications related to peripheral vasopressor administration is, therefore, more likely driven by factors related to vein integrity, PIV insertion and monitoring techniques rather than drug dose, concentration and duration of infusion. Threshold limits based on drug and infusion characteristics may not meaningfully reduce the numerical risk of peripheral vasopressor administration but might serve instead to reduce the risk of clinically significant tissue injury should extravasation happen, although robust evidence supporting this approach remains limited. Importantly, the absence of a demonstrated dose– or duration–response relationship in the published literature should not be interpreted as evidence of absence of risk, particularly given the small sample sizes, short follow-up periods and limited high-dose exposures in the available studies. Clinicians should, therefore, interpret the apparent dose and duration independence of complication rates with caution and continue to consider central access for low- (<0.5 µg/kg/min) and moderate-dose vasopressor therapy (e.g. norepinephrine equivalent doses of ≥0.5–0.7 µg/kg/min).
Peripheral administration of other vasopressors including vasopressin
While norepinephrine is the most studied and discussed vasopressor for PIV infusion, non-norepinephrine direct-acting catecholaminergic agents such as epinephrine, phenylephrine, dopamine and metaraminol were included in many studies.8,9 Overall, the safety profiles of these medications are likely similar to that of norepinephrine, and clinical considerations for PIV- or CVC-based infusion of these medications are not different.26,35
In contrast, vasopressin has additional considerations for the safety of peripheral administration. Its non-adrenergic mechanism of action through the V1 receptor on vascular smooth muscle makes it a useful and common adjunct in catecholamine-refractory shock.36 This mechanism of action and usage profile, however raises concern for its peripheral administration, due to the lack of a proven antidote. Moreover, patients with a need for vasopressin may have an increased rationale for a CVC (i.e. refractory shock, more than one vasopressor agent, escalating norepinephrine dose). The balance of evidence is currently uncertain for peripheral vasopressin: serious cases of vasopressin-related ischemic necrosis through both PIVs and CVCs have been reported, while other retrospective observational studies report a low risk of complications.10,37–39 Reflecting this uncertainty, almost all surveyed Michigan hospitals with peripheral vasopressor policies prohibited peripheral vasopressin.28 Caution is advised at this juncture pending further targeted study, except in emergency settings, while awaiting central access.
Clinical considerations
Protocolization of care
Peripheral initiation of vasopressors is a practice now supported by recent guideline recommendations from the Society of Critical Care Medicine and the Intensive Care Society.35,36 Currently, hospital protocols for the administration of peripheral vasopressors are heterogeneous, likely driven by the mixed data presented above and the lack of clear dose and duration thresholds.28 We suggest that local care contexts, including hospital systems and acute care networks, develop and institute rigorous protocols for peripherally administered vasopressors to reduce the risk and severity of complications and standardize the management of complications. General guidelines for policy development are outlined in Table 2, and input should be sought during guideline development from practitioners involved in the insertion, maintenance and monitoring of peripheral catheters. At our own institution, we use a decision framework similar to what is outlined in Figure 2, which may form the basis for similar institution-specific clinical decision protocols.5,30 At minimum, protocols should dictate what constitutes an acceptable PIV for peripheral vasopressor administration, the frequency and degree of monitoring for on-going use, limitations for the dose, duration and concentration of vasopressor agents, and a priori thresholds for escalation to CVC placement.
Table 2: General criteria for selecting initial vascular access for vasopressor administration
| PIV-based administration is generally appropriate when:
|
| Early CVC placement may be preferable when:
|
CVC = central venous catheter; PIV = peripheral intravenous.
Figure 2: Example clinical decision algorithm for peripheral vasopressors5,30
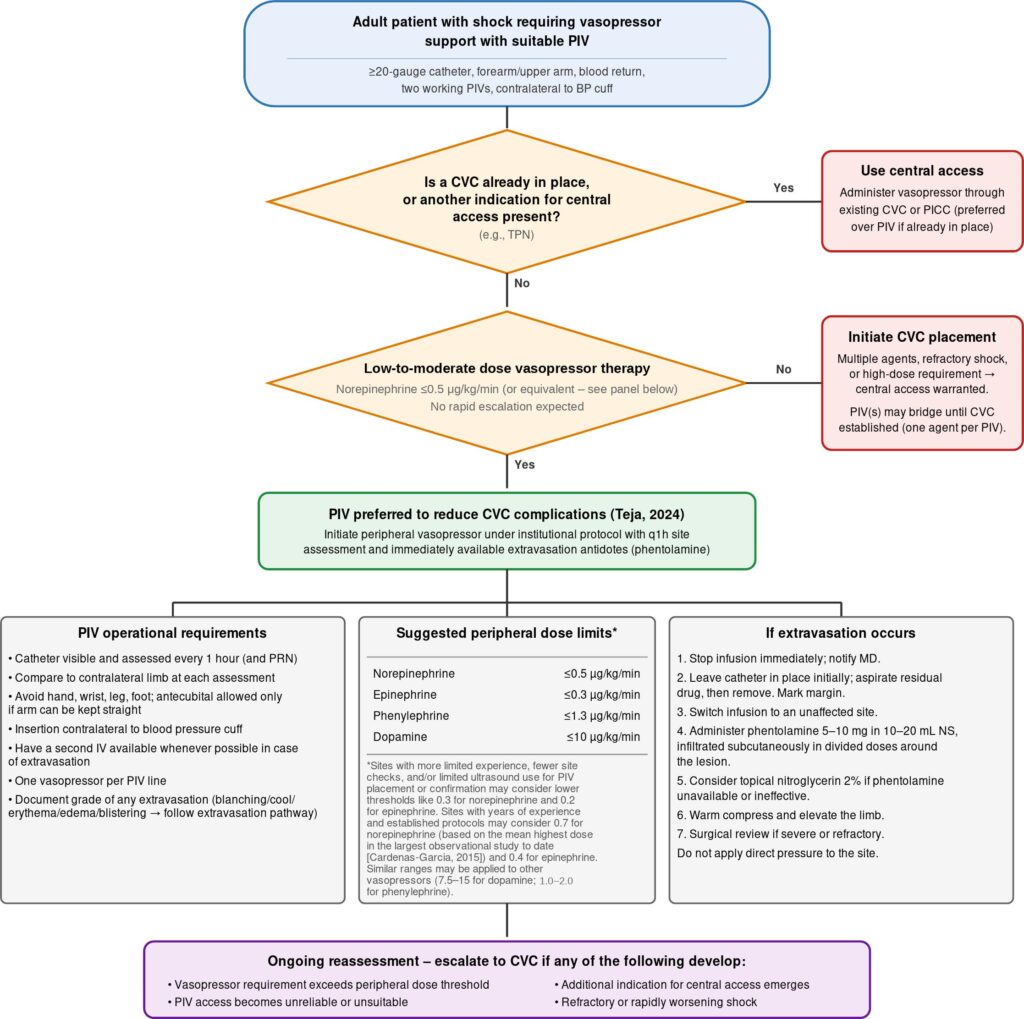
Dose thresholds are guideline-based suggestions; clinical judgement should always be exercised. Factors favouring continuation above threshold include anticipated near-term reduction in requirement (e.g. resolving hypervolemia, weaning sedation) or anticipated difficulty with CVC insertion
BP = blood pressure; CVC = central venous catheter; IV = intravenous; MD = physician; NS = 0.9% sodium chloride; PICC = peripherally inserted central catheter; PIV = peripheral intravenous catheter; PRN = pro re nata (as needed); q1h = every 1 h; TPN = high osmolality total parenteral nutrition.
Management of extravasation
In the event of extravasation events, it is critical to minimize the risk of progression to tissue ischemia and necrosis. Many of the studies demonstrating the safety of peripheral vasopressor infusions occurred in settings that mandated protocolized PIV catheter monitoring and the immediate availability of relevant antidotes and providers trained in their administration (Figure 1). We argue that these provisions are necessary to achieve conditions for the safety of peripheral vasopressor infusions.
Antidote therapy for vasopressor infiltration is most described for norepinephrine but likely applies to all direct-acting adrenergic vasoactive agents. As above, vasopressin has no known antidote therapy. To our knowledge, there are no RCTs on the management of established vasopressor infiltration; management largely reflects physiological rationale and practice standards (Table 3).40–43 Extravasation injuries secondary to non-vasoactive medications, such as chemotherapy and hyperosmolar agents, differ in management and are not discussed here.
Table 3: Management of vasopressor extravasation40–42
|
PIV = peripheral intravenous.
Alternative catheters for delivering vasopressor infusions
In addition to CVCs and PIVs, midline catheters (‘midlines’) and peripherally inserted central catheters (PICCs) can be used to infuse vasopressors and other medications. Midlines are peripherally inserted catheters that range in length from 6 to 20 cm. Often, cannulation is of the basilic, brachial or cephalic veins, with the catheter terminating in the axillary vein or even more distally in the upper arm.44 Their length allows for decreased extravasation risk.45,46 A 2022 retrospective study found no extravasation events among 203 patients with a combined 7,058 h of vasopressor infusion through a midline.47 However, extravasation events could theoretically be more severe due to deeper catheter termination, leading to deeper plane tissue injury and increased difficulty of recognizing injury. Given the more proximal catheter termination, the risk of venous thromboembolism (VTE) is likely increased as compared with PIVs; a meta-analysis including four studies using midline catheters for vasopressor infusion showed a pooled incidence of VTE of 1.4% (95% CI: 0.4, 5.4%).
PICCs are similarly inserted into the arm but terminate within the central circulation. They are often indicated for IV access for longer than 14 days or for therapies that strictly require central delivery.48 Peripheral placement eliminates the risk of life-threatening mechanical complications associated with CVCs, such as pneumothorax or hemothorax.49 Unsurprisingly, compared with PIVs, PICCs have an increased risk of VTE and CLABSI (0–12 per 1,000 catheter-days).50–52 Downstream sequelae of VTE-associated subclavian venous stenosis can be clinically impactful for certain populations, such as those with kidney disease; a case–control study of 120 patients with end-stage kidney disease showed an association between lack of functioning arteriovenous fistula and prior PICC use (odds ratio, 3.2; 95% CI: 1.9, 5.5, p<0.001) and the National Kidney Foundation’s Kidney Disease Outcomes Quality Initiative Guidelines on vascular access cautions against PICCs in patients with CKD.53–55
Midline and PICC catheters are best framed within the PIV-versus-CVC decision space described above rather than as stand-alone options: midlines may be considered as sitting alongside peripheral lines, with use directed when anticipated vasopressor duration exceeds typical PIV dwell times, but the clinical scenario does not otherwise mandate central access, whereas PICCs sit alongside CVCs as central-like options with a distinct insertion-complication profile. Given the limited prospective comparative data on the use of these catheter types for vasopressors, future studies should also specifically evaluate midline catheters as intermediate options between PIVs and CVCs for patients with anticipated longer-duration vasopressor requirements, with particular attention to extravasation rates, line-associated infection and patient-centered outcomes.
Conclusion
The historical preference for CVCs for vasopressor administration originated from an era defined by rudimentary catheter design and limited monitoring practices.2 While early cases of ischemia and necrosis from peripheral vasopressors understandably shaped decades of heightened caution, more contemporary evidence paints a markedly different picture.
Modern data demonstrate that peripheral vasopressor therapy carries a low risk of complications, the overwhelming majority of which are mild and self-limited.8,9,46,56 The risk of complications has not been shown to scale with vasopressor dose, duration or concentration, although this requires further investigation; importantly, the apparent absence of a dose– or duration–response relationship should not be interpreted as evidence of absence of risk, particularly at higher doses or longer durations. Modifiers of risk are likely related to catheter insertion technologies and techniques, anatomic considerations, protocolized monitoring and availability of antidote administration to prevent progression of minor complications to tissue injury requiring further intervention. Conversely, advances in technologies such as POCUS have also diminished the procedural risks of CVC insertion. However, residual risks associated with CVCs, such as VTE and CLABSI, are clinically important and almost always require additional therapies such as anticoagulation or antibiotics.
Overall, the current balance of the evidence argues that PIV-based vasopressor administration is a favorable first-line strategy for appropriately selected patients with adequate monitoring and institutional protocols in place, while CVC placement remains preferable for high-dose vasopressor therapy, multiple incompatible infusions or when indicated for other reasons (e.g. high osmolality TPN).


