
Despite significant advances over the years in cancer care, lung cancer unfortunately remains the leading cause of cancer-related mortality and one of the overall leading causes of death in the USA.1 Understanding the complex interaction between our patients and their clinical outcomes is important in facilitating the right approach to their care. Lung cancer has rightfully gotten significant attention in the context of the older population, especially regarding the association of racial and other socioeconomic factors with survival. It is known that racial minorities in the USA who are diagnosed with lung cancer face worse outcomes because they are less likely to be diagnosed early.2 Despite this, there exists a knowledge gap regarding these disparities in lung cancer incidence and survival outcomes, along with social and clinicopathological features among the adolescents and young adults (AYAs), an often-overlooked demographic.3
The adolescent and young adult stage typically refers to individuals between the ages of 15 and 39 years and represents a key developmental period marked by various psychosocial and healthcare challenges during the transition to adulthood. Traditionally, research has centred on cancers affecting children and older adults, resulting in a lack of comprehensive investigation and depth of knowledge into the challenges posed by cancer in AYAs. Recognizing and addressing disparities during this important phase is essential for strengthening the goals of early detection, personalized treatment and improved survival rates among all AYAs diagnosed with lung cancer.
This study aimed to highlight important changes in socioeconomic factors, incidence trends and survival disparities faced by AYAs from various racial backgrounds affected by lung cancer.
Methods
We performed a retrospective cohort analysis using data from the Surveillance, Epidemiology, and End Results (SEER, Surveillance Research Program, National Cancer Institute, Bethesda, MD, USA, SEER*Stat software, version 8.4.3).4 Research Plus Database, 17 Registries (2000–2020), which covers approximately 26.5% of the American population. We identified cases of lung cancer among individuals aged 15–39 years (AYAs) using the International Classification of Diseases for Oncology, Third Edition (ICD-O-3) codes listed in Supplementary Materials 1.5
To ensure data completeness and diagnostic accuracy, we included only cases with microscopic or laboratory confirmation of malignancy. Patients were excluded if they had unknown race, missing cause of death or non-confirmed diagnoses. We extracted the following variables from the SEER database:
-
Demographics: sex, race/ethnicity (White, Black, Asian/Pacific Islander, American Indian/Alaska Native or other/unknown) and age at diagnosis.
-
Tumour characteristics: histologic subtype and stage at diagnosis.
-
Socioeconomic factors: income level and urban versus rural residence.
-
Survival outcomes: survival in months, vital status and cause-specific death.
Descriptive statistics, including frequencies and medians, were used to summarize the characteristics of AYA lung cancer cases. Comparisons between AYAs and older adults were made using the chi-squared test for categorical variables.
Relative survival, defined as the observed survival among AYAs compared with expected survival in the general American population matched by age, sex and race, was estimated using SEER Stat software. Survival differences were further stratified by sex and race/ethnicity.
To identify factors independently associated with overall survival, we conducted Cox proportional hazards regression analyses separately for AYAs and older adults. Variables included in the models were demographic, clinical and treatment-related factors. Hazard ratios with 95% confidence intervals (CIs) were calculated, and a two-sided p-value of <0.05 was considered statistically significant.
Results
Baseline characteristics
Among the study cohort (see Table 1), which comprised 5,129 cases, 49.1% (n=2,519) were male and 50.9% (n=2,610) were female. Of these cases, 56.6% (n=2,904) were non-Hispanic White (NHW), 17% (n=872) Hispanic, 13.3% (n=684) non-Hispanic Black (NHB), 12.5% (n=643) non-Hispanic Asian or Pacific Islander (NHAPI) and 0.5% (n=26) non-Hispanic American Indian/Alaska Native (NHAIA). Disparities were noted in income status and area of residence, with a greater prevalence of lung cancer among individuals with higher income (≥$60,000) and those residing in metropolitan areas (p=0.001). The highest percentage of cancer was observed among NHAPI individuals with income >$75,000.
Table 1: Demographic and clinical characteristics of lung cancer in adolescents and young adults
| Demographic and clinical characteristics of lung cancer in AYA | |||||||
|
| All n (%) | NHW n (%) | NHB n (%) | Hispanic (all races) n (%) | NHAPI | NHAIA n (%) | p-value |
| Age, years | |||||||
|
| 36 (15–39) | 36 (15–39) | 36 (15–39) | 34 (15–39) | 35 (15–39) | 36 (21–39) | 0.001 |
| Sex | |||||||
| Overall | 5,129 (100.0) | 2,904 (100.0) | 684 (100.0) | 872 (100.0) | 643 (100.0) | 26 (100.0) | 0.228 |
| Male | 2,519 (49.1) | 1,411 (48.6) | 364 (53.2) | 426 (48.9) | 306 (47.6) | 12 (46.2) | |
| Female | 2,610 (50.9) | 1,493 (51.4) | 320 (46.8) | 446 (51.1) | 337 (52.4) | 14 (53.8) | |
| Income Status (Annual, household) | |||||||
| <US$35,000 | 72 (1.4) | 65 (2.1) | 7 (1.0) | 3 (0.3) | 0 (0.0) | 0 (0.0) | 0.001 |
| US$35,000–US$59,999 | 1,161 (22.6) | 762 (26.2) | 234 (34.2) | 132 (15.1) | 24 (3.7) | 9 (34.6) | |
| US$60,000–US$74,999 | 1,739 (33.9) | 892 (30.7) | 236 (34.5) | 406 (46.6) | 198 (30.8) | 7 (26.9) | |
| US$75,000 and above | 2,157 (42.1) | 1,188 (40.9) | 207 (30.3) | 331 (38.0) | 421 (65.5) | 10 (38.5) | |
| Area of residence | |||||||
| Missing/unknown | 4 | 0 | 0 | 0 | 0 | 4 | 0.001 |
| Non-metropolitan | 608 (11.9) | 504 (17.4) | 60 (8.8) | 30 (3.4) | 11 (1.7) | 3 (13.6) | |
| Metropolitan | 4,517 (88.1) | 2,400 (82.6) | 624 (91.2) | 842 (96.6) | 632 (98.3) | 19 (86.4) | |
|
| |||||||
| Types of lung cancer | |||||||
| Non-small cell cancer | 4,788 (93.4) |
|
|
|
|
| 0.001 |
| Squamous | 315 (6.1) | 180 (6.2) | 43 (6.3) | 48 (5.5) | 37 (5.8) | 7 (26.9) | |
| Adenocarcinoma | 2,232 (43.5) | 1,069 (36.8) | 301 (44.0) | 413 (47.4) | 439 (68.3) | 10 (38.5) | |
| Large cell | 153 (3.0) | 99 (3.4) | 31 (4.5) | 10 (1.1) | 12 (1.9) | 1 (3.8) | |
| Carcinoid tumour | 1,104 (21.5) | 752 (25.9) | 111 (16.2) | 207 (23.7) | 31 (4.8) | 3 (11.5) | |
| Others | 984 (19.2) | 560 (19.3) | 151 (22.1) | 158 (18.1) | 111 (17.3) | 4 (15.4) | |
| Small cell cancer | |||||||
|
| 341 (6.6) | 244 (8.4) | 47 (6.9) | 36 (4.1) | 13 (2.0) | 1 (3.8) | |
| Stage of cancer | |||||||
| Missing/unknown | 107 | 59 | 13 | 22 | 12 | 1 | 0.001 |
| Localized (I/II) | 1,133 (22.6) | 760 (26.7) | 104 (15.5) | 194 (22.8) | 72 (11.4) | 3 (12.0) | |
| Regional (III) | 975 (19.4) | 603 (21.2) | 150 (22.4) | 145 (17.1) | 71 (11.3) | 6 (24.0) | |
| Distant (IV) | 2,914 (58.0) | 1,482 (52.1) | 417 (62.1) | 511 (60.1) | 488 (77.3) | 16 (64.0) | |
| Time to initial treatment (chemotherapy/radiation/surgery) | |||||||
| Missing/unknown | 471 | 214 | 94 | 87 | 71 | 5 | 0.016 |
| <1 month | 2,255 (48.4) | 1347 (50.1) | 259 (43.9) | 373 (47.5) | 263 (46.0) | 13 (61.9) | |
| 1–3 months | 2,281 (49.0) | 1,289 (47.9) | 310 (52.5) | 386 (49.2) | 288 (50.3) | 8 (38.1) | |
| >3 months | 122 (2.6) | 54 (2.0) | 21 (3.6) | 26 (3.3) | 21 (3.7) | 0 (0.0) | |
| Survival in months | |||||||
| (Months) | 19 (0–251) | 20 (0–251) | 13 (0–250) | 20 (0–251) | 19 (0–251) | 7 (0–226) | 0.001 |
| Vital status | |||||||
| Alive | 2,094 (40.8) | 1,225 (42.2) | 221 (32.3) | 427 (49.0) | 213 (33.1) | 8 (30.8) | 0.001 |
| Dead | 3,035 (59.2) | 1,679 (57.8) | 463 (67.7) | 445 (51.0) | 430 (66.9) | 18 (69.2) |
|
| Cause of death | |||||||
| Missing/unknown | 60 | 12 | 6 | 21 | 20 | 1 | 0.043 |
| Due to lung cancer | 1,561 (93.6) | 1,561 (93.6) | 423 (92.6) | 403 (95.0) | 398 (97.1) | 16 (94.1) | |
| Due to other cancers | 106 (6.4) | 106 (6.4) | 34 (7.4) | 21 (5.0) | 12 (2.9) | 1 (5.9) | |
| Due to non-cancer causes | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | |
AYA = adolescents and young adults; NHAIA = non-Hispanic American Indian/Alaska Native; NHAPI = non-Hispanic Asian or Pacific Islander; NHB = non-Hispanic Black; NHW = non-Hispanic White.
Pathologic characteristics
Significant variations were observed in the distribution of histologic types of lung cancer among individuals of different racial and ethnic groups (p=0.001). Non-small cell lung cancer (NSCLC) as a group was markedly more common than small cell lung cancer (SCLC), accounting for 93.4% of the total cases (Table 1). Among NSCLC subtypes, adenocarcinoma was the predominant histologic subtype, accounting for 43.5% (n=2,232) of all cases, and this difference persisted when stratified by race and ethnicity. The highest percentage of adenocarcinoma was observed in the NHAPI population at 68.3% (p=0.001). The highest percentage of SCLC was seen among NHW individuals at 8.4% (p=0.001). The overwhelming majority of the population was diagnosed at stage III/IV, with NHAPI individuals having the highest percentage diagnosed at stage IV (77.3%, p=0.001).
Incidence rates and trends
The incidence rate per 100,000 was 11.04 (95% CI, 10.92–11.16) for men and 24.54 (95% CI, 24.36–24.72) for women. This difference in rate persisted across the racial/ethnic subgroups studied. The highest incidence was observed among the NHAIA subgroup at 21.5 (95% CI, 20.22–22.84), with females in this group more affected than males (Figure 1).
Figure 1: Incidence rates of lung cancer in adolescents and young adults stratified by sex and race
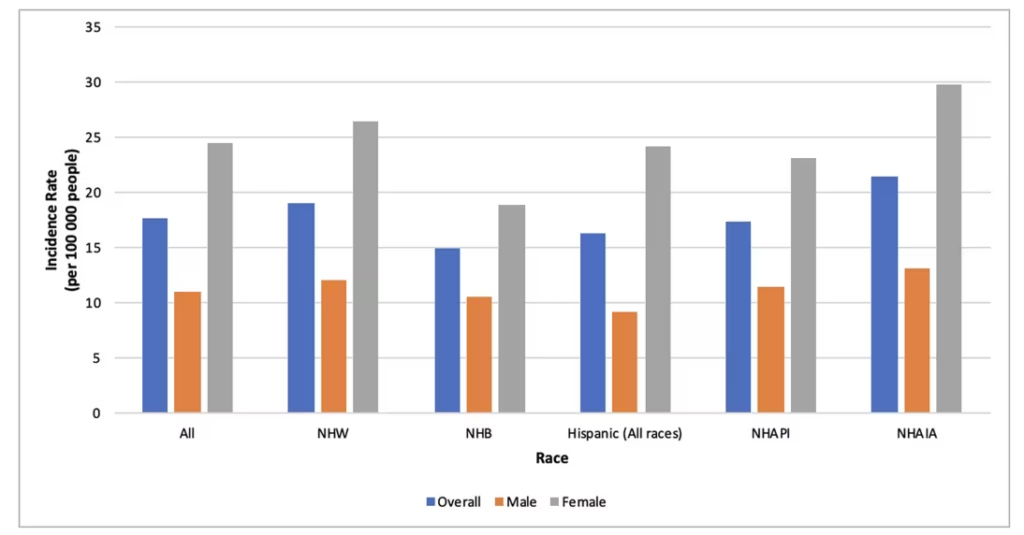
AYA = adolescents and young adults; NHAIA = non-Hispanic American Indian/Alaska Native; NHAPI = non-Hispanic Asian or Pacific Islander; NHB = non-Hispanic Black; NHW = non-Hispanic White.
Overall age-adjusted incidence rate (AAIR) of lung cancer among AYAs decreased (APC, −2.01 [–2.72 to –1.34]), slightly more in females (APC, –2.05 [–2.93 to –1.26]) compared with males (APC, –2.01 [–2.74 to –1.34]). The greatest overall decrease was observed among individuals identified as NHW (APC, –2.40 [–3.10 to –1.80]). There was no significant change in the AAIR among the NHB and Hispanic populations (Figure 2).
Figure 2: Age-adjusted incidence rates of lung cancer in adolescents and young adults (2000–2020)
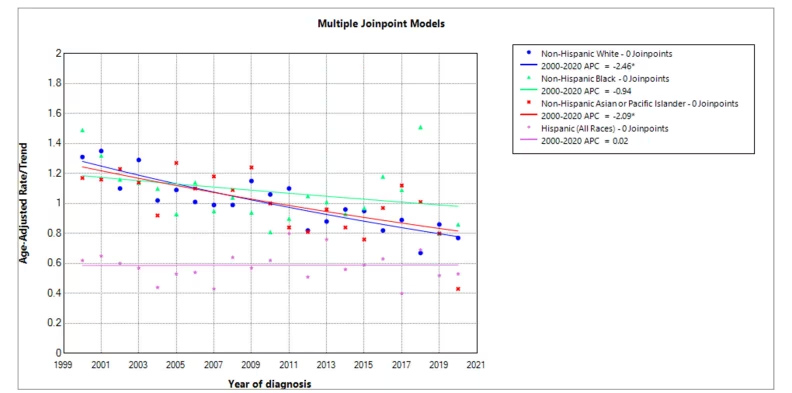
Joint Point Programme showing age-adjusted incidence rates of lung cancer in AYAs based on race between 2000 and 2020.
APC = annual percentage change; AYA = adolescents and young adults.
Survival
Survival analysis revealed differences in relative survival across the various racial and ethnic groups and sexes, with the overall lowest survival rate observed among individuals identified as NHAPI (RSR, –5: 28.7% [95% CI, 24.8–32.7%]). When stratified by sex, the lowest survival rate was seen among NHB men (RSR, –5: 25.60% [95% CI, 21.0–30.5%]), while the highest survival rate was observed among Hispanic women (all races) (RSR, –5: 48.1% [95% CI, 42.7–53.2%]; Table 2).
Table 2: Relative survival among adolescents and young adults with lung cancer
|
| NHW (% [95% CI]) | NHB (% [95% CI]) | NHAIA (% [95% CI]) | NHAPI (% [95% CI]) | Hispanic (all races) (% [95% CI]) |
| Overall | 43.2% [41.3–45.1%] | 31.3% [28.8–35.1%] | 30.9% [14.5–48.9%] | 28.7% [24.8–32.7%] | 44.6% [40.8–48.2%] |
| Male | 39.70% [37–42.4%] | 25.60% [21.0–30.5%] | 33.6% [10.3–59.2%] | 25.9% [20.5–31.5%] | 41.0% [35.8–46.2%] |
| Female | 46.6% [43.9–49.2%] | 37.8% [32.0–43.5%] | 28.0% [8.2–52.3%] | 31.2% [25.6–36.8%] | 48.1% [42.7–53.2%] |
AYA = adolescents and young adults; NHAIA = non-Hispanic American Indian/Alaska Native; NHAPI = non-Hispanic Asian or Pacific Islander; NHB = non-Hispanic Black; NHW = non-Hispanic White.
Discussion
In this study, we found significant variations in incidence trends, demographic patterns and survival outcomes of lung cancer in AYAs when stratified by race and ethnicity. In our study, we observed that AYAs tend to have NSCLC more frequently than SCLC, with NSCLC accounting for about 93.4% of cases. This is in keeping with the previous studies in other populations, where NSCLC is responsible for about 85% of cases of lung cancer.6
Within the NSCLC group, adenocarcinoma occurs more frequently than any other histological type. Rich et al. found that about 48% of AYAs with NSCLC have adenocarcinoma, which is similar to our findings, where 43.5% of AYAs with lung cancer have adenocarcinoma.7 Of note, the predominance of adenocarcinoma remained evident when stratified by race and ethnicity, with the highest percentage seen among individuals identified as NHAPI.
Multiple factors likely contribute to the predominance of adenocarcinoma in its incidence as a lung cancer subtype. While the link between all types of lung cancer and smoking is widely established, adenocarcinoma remains the most common subtype of lung cancer seen in nonsmokers as well, suggesting that there are other, less well-known risk factors (such as radon, cooking fumes and asbestos exposure) that may predispose AYAs to adenocarcinoma.8–10 Adenocarcinoma is also associated with several genetic mutations that are less frequent in other types of lung cancer. These mutations often occur in genes like EGFR (epidermal growth factor receptor), KRAS (Kirsten rat sarcoma viral oncogene homologue) and ALK (anaplastic lymphoma kinase), perhaps adding to an ever-growing list of risk factors for disease development and hence its prevalence.11,12 Our study revealed the highest percentage of adenocarcinoma among NHAPI individuals, which may be explained by many of the aforementioned factors, particularly with one study showing that as many as 90% of East Asian nonsmokers diagnosed with adenocarcinoma tested positive for one of numerous oncogenes such as EGFR, KRAS, ALK, HER2 (human epidermal growth factor receptor 2), BRAF (v-raf murine sarcoma viral oncogene homologue B1) and RET (rearranged during transfection).13
The incidence of lung cancer in AYAs with higher income and those who lived in metropolitan areas was remarkably higher. This represents a deviation from previous studies, which showed that low socioeconomic status (SES) and rural area of residence are associated with increased risk of lung cancer development, and even after adjustment for smoking, it remained an independently significant risk factor.14,15 This divergence in our results is possibly explained by the fact that individuals with higher SES generally have better access to healthcare services, including preventive screenings and early detection programmes, leading to earlier/higher rates of detection of lung cancer.16 Urban environments can also be associated with higher levels of air pollution.17 Moreover, certain occupations associated with metropolitan areas, such as construction and manufacturing, may involve exposure to carcinogens and thus increase the risk of lung cancer among such individuals.10,18
Our study also showed that the overall AARI of lung cancer is decreasing across all racial/ethnic groups, except in individuals identified as NHB and Hispanic, prompting further exploration into potential underlying factors. The decreasing overall incidence rate noted is consistent with previously published articles that identify a similar decrease.19 One possible explanation for this overall decrease could be linked to lifestyle modifications such as decreased cigarette smoking, likely as a result of public health campaigns, increased awareness about the dangers of smoking and initiation of smoking cessation programmes.20 Smoking is the leading cause of lung cancer; hence, a reduction in smoking rates can directly lead to a decrease in lung cancer cases.8 However, while cigarette smoking is the paramount risk factor for the development of lung cancer, it is important to consider that the protracted duration necessary for the manifestation of lung cancer due to smoking may render it less discernible in AYAs. Perhaps, efforts to reduce exposure to environmental carcinogens such as radon, asbestos and other forms of air pollution may also contribute to the decline in lung cancer rates, as regulations on workplace safety and environmental protection are more stringent than in years past since the inception and growth of institutions like the Environmental Protection Agency and the Occupational Safety and Health Administration.21 Among the general NHB/Hispanic population, previous studies showed an increase in rates among NHBs and a decline among Hispanics.22,23 Explanations for the lack of change in incidence among NHBs and Hispanics in our study could be multifaceted and may involve various socioeconomic, cultural and healthcare access-related factors. For instance, disparities in healthcare access and utilization could be a contributing factor. One study revealed that not only are certain vulnerable populations limited in their access to healthcare but they are also often underrepresented in clinical trials, data gathering and other healthcare innovations.24 Additionally, genetic predispositions and environmental exposures may also play a role in influencing disease incidence among NHB and Hispanic populations.22 Further research into these factors is warranted to gain a comprehensive understanding of the observed patterns and to inform public health interventions aimed at reducing cancer incidence across diverse ethnic groups.
Overall, NHAPI individuals had the lowest survival rate among all racial and ethnic groups, with about the same percentage as one prior study at 26.7%.25 One possibility is that patients in this group, most of whom have minimal tobacco exposure, often test positive for various proto-oncogenes such as EGFR, RET and ALK, which may be the drivers of aggressive variants of lung cancer – as with prior studies showing that EGFR, KRAS and RET mutations are more frequently seen in certain patterns of intrapulmonary metastases, indicating a potential correlation with poor prognosis.26–29
The observed disparities in survival among NHB men confirm the findings of prior studies.30 Many factors may contribute to this concerning trend, including limited access to healthcare services, financial barriers and lower rates of health insurance coverage among Black populations, as well as cultural mistrust of the healthcare system and lower participation in preventive screening programmes, which may delay diagnosis and treatment initiation, leading to more advanced disease stages at presentation.30,31 Furthermore, biological differences, including variations in tumour biology and genetic predispositions, may also play a role in tumour aggressiveness and response to therapy, with one study showing differences in tumour biology between African Americans and European Americans.32
Limitations
This study has some limitations, including its retrospective nature, observational design and the use of registry data that may lack important risk factors such as smoking, family history, oncogenic mutations and adequate treatment data on immunotherapy. Despite these limitations, the SEER database provides the advantage of being a nationwide, comprehensive repository covering young adults diagnosed with lung cancer in the USA over a 20-year period. Therefore, our findings offer a valuable and thorough update on the epidemiology of lung cancer among AYAs.
Conclusion
We found a decreasing overall AAIR of lung cancer across all racial/ethnic groups, although not statistically significant in individuals identified as NHB and Hispanic, suggesting a need for further exploration into potential underlying factors. Additionally, we observed a predominance of NSCLC over SCLC in AYAs, with adenocarcinoma being the most common histological type across all racial/ethnic groups, with the highest rates seen among NHAPI individuals. The higher incidence of lung cancer in AYAs with higher income and those living in metropolitan areas diverges from previously established risk factors, likely due to better access to healthcare screening services and increased exposure to environmental carcinogens. Furthermore, disparities in 5-year survival among NHAPI individuals overall and NHB men highlight the need for addressing healthcare access barriers and cultural factors to achieve more equitable outcomes.









