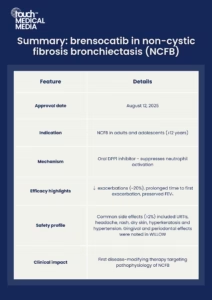
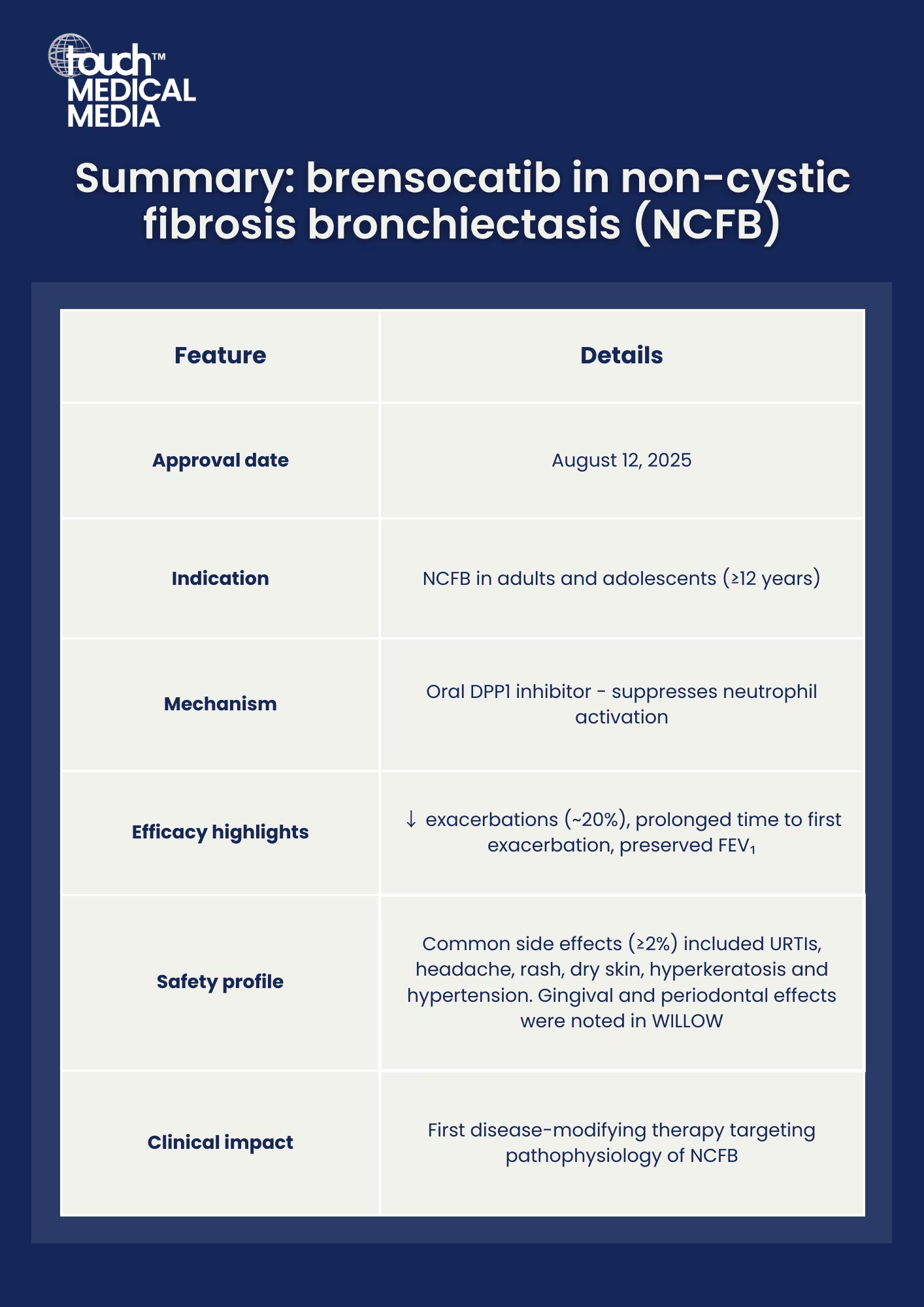
On August 12, the FDA granted approval to brensocatib, making it the first and only therapy specifically indicated for non-cystic fibrosis bronchiectasis (NCFB).1,2,3 NCFB is a chronic, progressive lung disease marked by permanently dilated bronchi, which leads to frequent pulmonary exacerbations. Symptoms of disease often include chronic cough, sputum overproduction, and frequent infections.
A long-awaited therapeutic option for patients
Brensocatib offers the first treatment specifically targeting the underlying inflammatory cause of NCFB, rather than managing symptoms alone. For the estimated 500,000 individuals in the US living with NCFB, the approval brings a “significant and long-awaited advancement”, as Elisha Malanga (Executive Director, Bronchiectasis and NTM Association) remarked, that may help people better manage the burden of disease and improve daily life.3
Mechanism of action: targeting neutrophil activation
Brensocatib is a small-molecule dipeptidyl peptidase 1 (DPP1) inhibitor, administered orally once daily. By inhibiting DPP1, brensocatib prevents activation of neutrophil serine proteases: key enzymes in neutrophil-driven inflammation and tissue damage in bronchiectasis.2
 Evidence from clinical trials: ASPEN and WILLOW
Evidence from clinical trials: ASPEN and WILLOW
Approval was supported by results from two pivotal studies:
- Phase III ASPEN trial (NCT04594369)4: Brensocatib demonstrated significant reductions in annualized exacerbation rates: 21.1% with 10mg and 19.4% with 25mg compared to placebo. Secondary benefits included prolonged time to first exacerbation and higher rates of patients remaining exacerbation-free. Patients receiving brensocatib had a smaller decline in lung function compared to placebo, as measured by post-bronchodilator FEV₁ at 52 weeks.
- Phase II WILLOW trial (NCT03218917)5: Brensocatib significantly prolonged the median time to first exacerbation: 134 days with 10mg and 96 days with 25mg, versus 67 days with placebo. Furthermore, brensocatib reduced the risk of exacerbations, with both doses also lowering sputum neutrophil elastase activity over 24 weeks. The 10mg dose also achieved a statistically significant 36% reduction in the rate of exacerbations compared to placebo.
Safety and tolerability
Common adverse events (≥2%) included upper respiratory tract infections, headache, rash, dry skin, hyperkeratosis, and hypertension. Safety findings were similar in both ASPEN and WILLOW, with the exception of the noted gingival/periodontal effects in the WILLOW study.3
Clinical implications: a new standard of care
In clinical practice, brensocatib provides the first approved pharmacologic option for NCFB, introducing a therapy that targets underlying neutrophilic inflammation rather than solely addressing symptoms. This approval represents not just a regulatory milestone but a tangible step forward for patients and clinicians alike in managing a complex, under-treated respiratory disease.
References
- AJMC. Brensocatib Becomes First FDA-Approved Therapy for Bronchiectasis. 2025. [Press release]. Available at: www.ajmc.com/view/brensocatib-becomes-first-fda-approved-therapy-for-bronchiectasis (accessed 15 August 2025).
- Pharmacy times. Brensocatib Becomes First Approved Treatment for Non-Cystic Fibrosis Bronchiectasis in Adults, Adolescents. 2025. [Press release]. Available at: www.pharmacytimes.com/view/brensocatib-becomes-first-approved-treatment-for-non-cystic-fibrosis-bronchiectasis-in-adults-adolescents (accessed 15 August 2025).
- Insmed. FDA Approves BRINSUPRI™ (brensocatib) as the First and Only Treatment for Non-Cystic Fibrosis Bronchiectasis, a Serious, Chronic Lung Disease. 2025. [Press release]. Available at: investor.insmed.com/2025-08-12-FDA-Approves-BRINSUPRI-TM-brensocatib-as-the-First-and-Only-Treatment-for-Non-Cystic-Fibrosis-Bronchiectasis,-a-Serious,-Chronic-Lung-Disease (accessed 15 August 2025).
- Chalmers J, Burgel PR, Daley C, et al. Phase 3 trial of the DPP-1 inhibitor brensocatib in bronchiectasis. N Engl J Med. 2025;392:1569–1581.
- Chalmers J, Haworth C, Metersky M, et al. Phase 2 trial of the DPP-1 inhibitor brensocatib in bronchiectasis. N Engl J Med. 2020;383:2127–2137.
Editor: Victoria Smith, Senior Content Editor.
Disclosures: This article was created by the touchRESPIRATORY team utilizing AI as an editorial tool (ChatGPT (GPT-4o) [Large language model]. https://chat.openai.com/chat.) The content was developed and edited by human editors. No funding was received in the publication of this article.
Cite: Approval of brensocatib marks a paradigm shift in bronchiectasis care. touchRESPIRATORY. 18 August 2025.
Related content
- Breaking the Vicious Vortex: Targeting Pseudomonas Aeruginosa Infection in Bronchiectasis – Insights from GREAT-2
- GINA 2025 Brings New Personalized, Proactive Changes to Asthma Care
- July respiratory medicine roundup: key regulatory decisions and clinical trial results
Register now to receive the touchRESPIRATORY newsletter!
Don’t miss out on hearing about our latest peer reviewed articles, expert opinions, conference news, podcasts and more.